

I am recently in the midst of completing the “Running Symposium” held in Australia – the first of its kind brought about by COVID. It has ran over three days and has guest lecturers from all over the world who are specialists in their fields which include running. When a topic came up about the myths surrounding osteoarthritis (OA) and running what are the recommendations, I had to listen and it has given me a greater understanding of the misconception surrounding running and increased “wear and tear” of the knee – if that is even a concept?!.
“Bone on Bone”
I have lost count the times clients/patients have came into the clinic and have been told to “stop running because they will wear out their knees” or “your knees won’t thank you for running” or “I am too old to start running it will just cause me knee pain” the list is not exhaustive.

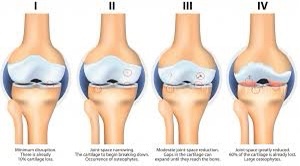
During this post I wanted to address some of the literature out there presented by Kevin Maggs about the misconceptions surrounding running and knee arthritis. He starts off by discussing the recent paper by Bunzli 2019 where patients awaiting orthopaedic surgery for Osteoarthitis of the knee were questioned about their beliefs to the pathology. Initially, the first question was ” what is osteoarthritis?” – the answer (every participant) stated bone on bone – which implies a structural origin. In a further study by Culvenor 2019 looked at ASYMPTOMATIC knees (no pain symptoms) and scanned these and found that there were a high rate of boney changes in the asymptomatic knees. So the question would be why do some people present with pain and some people don’t whilst both groups have structural changes? Yusuf 2011 then went on to try and link findings from an MRI to the association of pain. Effusion and synovitis at 86% and bone marrow lesions at 63% (both inflammatory) were the highest correlation factors linking to pain that were found on the MRI.
Pain however is complex and multifactorial. Neogi 2009 linked previous experience, genetics, expectations, current mood and coping strategies with expected outcome. So rather than comparing multiple knees they suggested comparing the affected vs the not affected leg, as all the multifactorial elements would be the same for that individual. They found that when the Kellgren-Lawrence scale (The KL classification was originally described using AP knee radiographs. Each radiograph was assigned a grade from 0 to 4, which they correlated to increasing severity of OA, with Grade 0 signifying no presence of OA and Grade 4 signifying severe OA ) differed the most between the affected leg and non affected leg, the worse pain symptoms were experienced.
The study summarised that pain in symptomatic knees was due to mix of inflammation rather ran structured defects alone in the knee. So bone on bone structural defects alone don’t cause the pain an inflammatory reaction and psychological handling of the symptoms causes the pain.
If not running then what causes OA?
Over 30 studies concluded that two of the biggest factors relating to knee osteoarthritis were fat mass/obesity and previous injury.

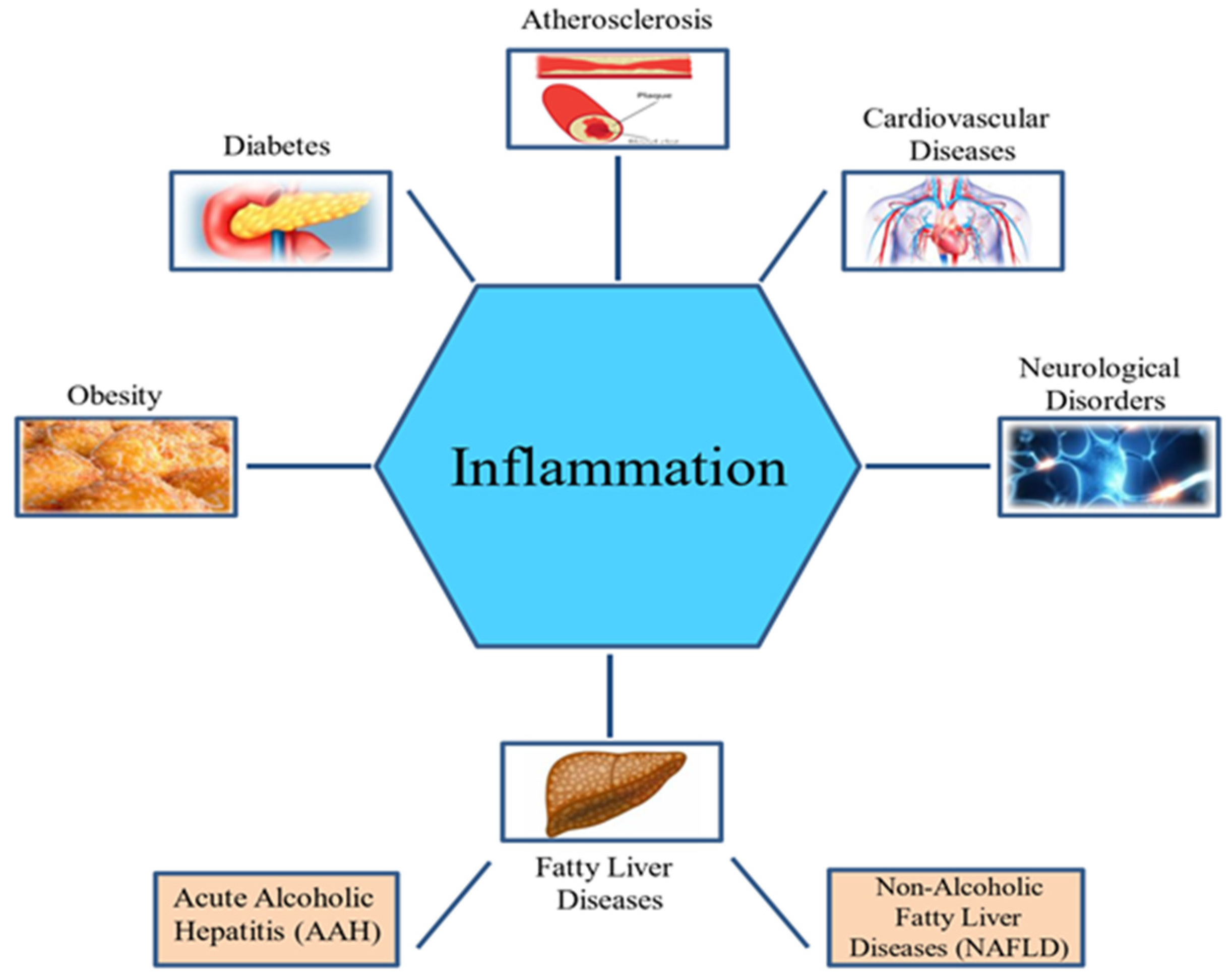
With an increased fatness/obesity you will have a larger mechanical load, i.e the muscles, bones, joints, tendons and cardiovascular system will have to work harder to move this mass. With an increased fat mass / obesity there is also a higher inflammatory response in the body. Linking to the previous section we know that the higher the inflammatory response the more you will likely be in pain from the loaded joints / muscles / tendons etc. Urban and Little 2018 summarise that the role of fat as an endocrine organ secreting an array of pro-inflammatory mediators. In other words promoting inflammation. In other words increasing the likely hood of symptoms of the knee in this case.

So the summary is that genetics, fat mass, hormones and previous injury affect the structure nature of the pathology. The mood, catastrophizing, inflammation and self efficacy effect the pain. The two over lap, so when addressing the pathology in the clinic structure shouldn’t be addressed on its own, and neither should the pain symptoms. So in fact structure matters but isn’t the whole picture.
“Wear and tear”?
The original study Bunzli 2019 the most sought answer was “wear and tear” of the joint. However, when we look at the physiological adaptations to load we don’t see the relationship. For example loading muscle brings improved strength and increased cross sectional area. Furthermore loading bone causes increased bone density through mechanotherapy. So the question arises why would applying load to a joint then cause a deleterious affect in “wear and tear’?

So what happens during running at the cartilage level. The compression reduces the volume of the water content in the cartilage. After waiting an hour after exercise it was found that the cartilage water content returned to pre exercise level (Kessler 2008). Because the body knows that the cartilage volume of water reduces exercise, it adapts to a consistent load by increasing the glycosaminoglycan content ( which helps to regulate the water content in the cartilage). Furthermore, studies have shown that exercise as an intervention has shown to increase the glycosaminoglycan content and like exercise that strengthens bone density and muscle cross sectional area, it can provide more efficient cartilage water reabsorption following exposure.
So far exercise not only has been shown to not cause osteoarthritis, the benefits of exercise are protective to the onset of osteoarthritis. Even if you have osteoarthritis, beginning / continuing an exercise intervention can help to manage the symptoms and aid pain management of the pathology (Over 12systematic reviews and counting).
When is too much exercise detrimental to knee osteoarthritis and in particular running?
There has been a link with directional changing sports with high prevelence of knee osteoarthritis over running. Football, association and American, along with weight lifting have shown greater levels of knee osteoarthritis versus running but there is a ceiling where the volume of running becomes detrimental and causative .

Lo 2019 compared runners to non runners in the development of osteoarthritis in a both groups as a cross sectional study. There was less radiographic and symptomatic knees in the running group compared to the non-running group. The same study went on to show that there was a dose dependant reaction in that the more the runner ran the less symptoms and pain they presented with. They summarised their study by stating that individuals that didn’t have osteoarthritis, running does not appear to be detrimental to knees.
A further study looking at the dose of running of elite running (miles over 100miles per week) compared to recreational ( 40-60miles per week) and control group (0 miles) on the prevalence of osteoarthritis in the knee and hip found the following. Elite runners presented the highest at 13.3%, followed by the control group at 10.2% and least affected were the recreational running at 3.5% (6.5% prevalence than the control group).

On a follow up study (Timmins 2017) at 25 years there was a 54% less surgical intervention in the recreational running group than the control group of non runners.
Lo (2018) further looked at over 50 year old participants with a diagnosis of Osteoarthritis in the knee to determine what the effects of running were on the knees. They found that running was not associated with worsening pain or structural changes over the study. In fact there was an improvement in the pain of the individuals who continued to run versus the non running group.
Thee studies would suggest that not only does running not show a link with causative factors of osteoarthritis, it can be used as a successful management tool if prescribed and managed correctly.

So how do we manage Osteoarthritis in the knee?
As previously mentioned the two things that can increase the risk and symptoms of osteoarthritis is the mechanical load on the joint and the level of inflammation surrounding the tissue of the joint. In patients that are over weight it was shown that a reduction of weight by 5-15% had significant positive outcomes on pain (Chu 2018), physical function (Chu 2018) and quality of life (Chu 2018).

The effect is dose dependant which means the more weight you lose the bigger the effect on the three markers above. The effect was only shown up until 12 months. After 12 months the benefit reduced as a dose dependant influence. This was due to the level of adherence with a training programme. Patients / subjects were good up to 12 months at sticking to the exercise prescription and weight loss was up to 11% (Hall 2008) but after 12 months the level of adherence dropped and the gain in weight was only 7% ( so the subjects had gained 5% of the initially lost weight) and this reduced the positive relationship with weight loss and pain, QOL and physical function. Diet a lone requires 15% weight loss to have a positive effect whilst diet and exercise you only need 6-8% weight loss to have a positive outcome.
Running in the Osteoarthritic patient: how can we adapt to continue?
The key way to continue to reap the benefits that exercise brings with the management of osteoarthritis is to remain active. To do this and continue running the patients to be educated on the pathology and why running is beneficial. They also require appropriate educational support from nutritionalist or weight management input.

As physiotherapists and through gait analysis like in the clinic you can manipulate the load that goes through the knee by altering the cadence of the runner. Increasing the cadence has been shown to reduce the load on the patellofemoral and knee joints. Increasing the cadence means that you will be in contact with the ground more often but the force in which you hit the ground will be less as there is less vertical displacement…thick of pole vaulter vs a skimming stone. We can also change the way the foot contacts the ground. Non-rearfoot striking places less load through the knee joint, but caution should be taken with this as it moves the load to else where in the body mainly gastrocnemius, soleus and achillies tendon.

The next thing that physiotherapists can do well is to build the capacity of the patient. Gradual increments in loading are important. This can be from step ups on progressively bigger steps to double leg bounding to skipping to single leg hopping to marching on the spot to jogging to a return or graduated run program like couch to 5 km.
With introducing running to the patient with osteoarthritis it is important to stick to main capacity measures. Firstly there maybe discomfort but no pain, with any discomfort dissipating by 60minutes after exercise finishes. There should be no swelling around the knee suggesting of inflammation of the joint. The patient shouldn’t have to compensate in normal day to day activities or limp following the programme and the volume followed by speed should be progressed whilst being mindful of these capacity measures.
Surgical Management
The figures from the patients undergoing total knee replacement showed that 90% of these were overweight or obese. From the total number of completed surgeries 20% (1 in 5) were not satisfied with the outcome of the operation ( Beswick 2012). Furthermore (Kulkarni 2016) of the completed surgeries that were performed on obese / overweight individuals, 1 in 3 (33%) were dissatisfied with the outcome of the surgery.

Summary
Knee osteoarthritis is not just a structural, it is inflammatory, psychosocial and structural so imaging will not be able to diagnosis it.

Knee osteoarthritis is not a wear and tear pattern. If it was exercise would not be a successful management intervention. Exercise is beneficial in the management of osteoarthritis of the knee by helping to control weight management and physiological changes but the adherence to lifestyle changes have to be maintained to continue to see the benefits of exercise.

Weight management is important in the management of osteoarthritis. It is also important in the success of any intervention both conservative and surgical and the education/adherence of the patient is pivotal for this to be effective.

The patient should manage their symptoms to how they feel rather than a medial professional telling them how to feel. Keep a positive mind-frame as this has a benefit on the outcome of interventions.
Run if they wish and work with parameters – it will help with weight management and lifestyle improvement.
There is no drug, in use or being developed, that shows as much promise to bring health to its users than a sustained exercise program
Walter Bortz
Thanks as always for reading
Run Long and Prosper
James
Comments are closed